The Centers for Medicare & Medicaid Services (CMS) issued the 2016 deductibles, coinsurance, and premium rates for beneficiaries covered through the Medicare fee for service program. The 2016 deductible, coinsurance and base premium rates are:
2016 Part A - Hospital insurance
Deductible: $1,288.00
Coinsurance
• $322 a day for 61st-90th day
• $644 a day for 91st-150th day (lifetime reserve days)
• $161 a day for 21st-100th day (skilled nursing facility coinsurance)
2016 Part B - Supplementary medical insurance (SMI)
Under Part B of the Medicare supplementary medical insurance (SMI) program, enrollees are subject to a monthly premium. Most SMI services are subject to an annual deductible and coinsurance (percent of costs that the enrollee must pay), which are set by statute.
Deductible: $166 a year
Coinsurance: 20 percent
Showing posts with label Medicare part B. Show all posts
Showing posts with label Medicare part B. Show all posts
Why physician should participate with Medicare
Medicare Participation for Calendar Year 2013
The importance and advantages of being a Medicare participating provider, and we are pleased that the favorable trend of participation continued into 2012 with a participate rate of
96.1 percent, the highest ever. As you plan for 2013 and become familiar with the coming changes, we are hopeful that you will continue to be a participating provider or, if you are non-participating, will consider becoming a participating provider.
As a reminder the following incentive programs are available for Medicare physicians in 2013:
• Certain primary care specialties, as authorized by the Affordable Care Act, may receive a 10 percent incentive payment for rendering primary care services;
• Electronic health record incentive payments will continue for eligible professionals who demonstrate meaningful use, and;
• Eligible professionals will continue to have the opportunity to earn incentive payments for participating in the Physician Quality Reporting System.
Please see below for more specific information regarding these programs.
WHY BECOME A PARTICIPATING MEDICARE PROVIDER
All physicians, practitioners and suppliers must make their CY 2013 Medicare participation decision by December 31, 2012. Providers who want to maintain their current participation (PAR) status (PAR or Non PAR) do not need to take any action during the upcoming annual participation enrollment program. To sign a participation agreement is to agree to accept assignment for all covered services that you provide to Medicare patients in CY 2013. The overwhelming majority of physicians, practitioners and suppliers have chosen to participate in Medicare. As indicated, during CY 2012,
96.1 percent of all physicians and practitioners are billing under Medicare participation agreements.
If you participate and you bill for services paid under the Medicare physician fee schedule, your
Medicare fee schedule amounts are 5 percent higher than if you do not participate.
In 2013, you will see a continuation of the Medicare program’s emphasis on primary care and important incentive and quality of care initiatives. Our goal of better health and better care at lower costs may be seen through a number of programs, some of which are described below.
Primary Care Incentives
In 2013, CMS will continue to make a 10 percent incentive payment for primary care services furnished by primary care practitioners as authorized by the Affordable Care Act. To be eligible for this incentive payment, a physician’s Medicare specialty needs to be family medicine, geriatric medicine, pediatric medicine, or internal medicine and primary care services needed to constitute 60 percent of Medicare Part B outpatient services (excluding services provided to hospital inpatients or those in emergency departments) in 2011. Nurse practitioners, clinical nurse specialists, and physician assistants are also eligible for these incentive payments. For the first time in 2013, Medicare payments will explicitly reflect the care required to help a patient transition back to the community following a discharge from a hospital or nursing facility. The new codes will recognize the additional resources required by the physician to coordinate a patient’s care following a hospital or nursing facility stay.
Incentives and Payment Adjustments for Quality Reporting
In 2013, eligible professionals (EPs) will have the opportunity to earn incentive payments equal to 0.5 percent of their total allowed Medicare Part B Fee-for-Service charges for services provided during
2013 under both the Physician Quality Reporting System (PQRS) and the Electronic Prescribing (eRx) Incentive Program. Incentive payments earned in 2013 will be paid in CY 2014.
EPs should note that 2013 will also serve as the reporting period for the PQRS payment adjustment that will be applied in 2015. The reporting requirements for the 2015 PQRS payment adjustment are detailed in the 2013 Medicare Physician Fee Schedule (MPFS) Final Rule. Payment adjustments will be applied in CY 2013 and CY 2014 to those EPs who are not successful electronic prescribers under the eRx Incentive Program. EPs can still avoid the 2014 eRx payment adjustment by (1) meeting the reporting requirements for purposes of the 2012 eRx incentive; or (2) reporting the eRx measure on at least 10 unique events from January 1, 2013, through June 30, 2013; or (3) requesting and being granted an exemption due to a significant hardship. CMS expects that EPs will be able to request hardship exemptions via the web in the summer/fall of 2013.
The importance and advantages of being a Medicare participating provider, and we are pleased that the favorable trend of participation continued into 2012 with a participate rate of
96.1 percent, the highest ever. As you plan for 2013 and become familiar with the coming changes, we are hopeful that you will continue to be a participating provider or, if you are non-participating, will consider becoming a participating provider.
As a reminder the following incentive programs are available for Medicare physicians in 2013:
• Certain primary care specialties, as authorized by the Affordable Care Act, may receive a 10 percent incentive payment for rendering primary care services;
• Electronic health record incentive payments will continue for eligible professionals who demonstrate meaningful use, and;
• Eligible professionals will continue to have the opportunity to earn incentive payments for participating in the Physician Quality Reporting System.
Please see below for more specific information regarding these programs.
WHY BECOME A PARTICIPATING MEDICARE PROVIDER
All physicians, practitioners and suppliers must make their CY 2013 Medicare participation decision by December 31, 2012. Providers who want to maintain their current participation (PAR) status (PAR or Non PAR) do not need to take any action during the upcoming annual participation enrollment program. To sign a participation agreement is to agree to accept assignment for all covered services that you provide to Medicare patients in CY 2013. The overwhelming majority of physicians, practitioners and suppliers have chosen to participate in Medicare. As indicated, during CY 2012,
96.1 percent of all physicians and practitioners are billing under Medicare participation agreements.
If you participate and you bill for services paid under the Medicare physician fee schedule, your
Medicare fee schedule amounts are 5 percent higher than if you do not participate.
In 2013, you will see a continuation of the Medicare program’s emphasis on primary care and important incentive and quality of care initiatives. Our goal of better health and better care at lower costs may be seen through a number of programs, some of which are described below.
Primary Care Incentives
In 2013, CMS will continue to make a 10 percent incentive payment for primary care services furnished by primary care practitioners as authorized by the Affordable Care Act. To be eligible for this incentive payment, a physician’s Medicare specialty needs to be family medicine, geriatric medicine, pediatric medicine, or internal medicine and primary care services needed to constitute 60 percent of Medicare Part B outpatient services (excluding services provided to hospital inpatients or those in emergency departments) in 2011. Nurse practitioners, clinical nurse specialists, and physician assistants are also eligible for these incentive payments. For the first time in 2013, Medicare payments will explicitly reflect the care required to help a patient transition back to the community following a discharge from a hospital or nursing facility. The new codes will recognize the additional resources required by the physician to coordinate a patient’s care following a hospital or nursing facility stay.
Incentives and Payment Adjustments for Quality Reporting
In 2013, eligible professionals (EPs) will have the opportunity to earn incentive payments equal to 0.5 percent of their total allowed Medicare Part B Fee-for-Service charges for services provided during
2013 under both the Physician Quality Reporting System (PQRS) and the Electronic Prescribing (eRx) Incentive Program. Incentive payments earned in 2013 will be paid in CY 2014.
EPs should note that 2013 will also serve as the reporting period for the PQRS payment adjustment that will be applied in 2015. The reporting requirements for the 2015 PQRS payment adjustment are detailed in the 2013 Medicare Physician Fee Schedule (MPFS) Final Rule. Payment adjustments will be applied in CY 2013 and CY 2014 to those EPs who are not successful electronic prescribers under the eRx Incentive Program. EPs can still avoid the 2014 eRx payment adjustment by (1) meeting the reporting requirements for purposes of the 2012 eRx incentive; or (2) reporting the eRx measure on at least 10 unique events from January 1, 2013, through June 30, 2013; or (3) requesting and being granted an exemption due to a significant hardship. CMS expects that EPs will be able to request hardship exemptions via the web in the summer/fall of 2013.
what is Medicare part B and who is covered
Part B – Medical Insurance
Some of the services that Part B, medical insurance, helps pay for include
: Medically necessary services furnished by physicians in a variety of medical settings, including but not limited to:
o The physician’s office;
o An inpatient or outpatient hospital setting; and
o Ambulatory Surgical Centers; Home health care for individuals who do not have Part A; Ambulance services; Clinical laboratory and diagnostic services; Surgical supplies; Durable medical equipment, prosthetics, orthotics, and supplies; Hospital outpatient services
; and Services furnished by practitioners with limited licensing such as:
o Audiologists;
o Certified nurse midwives;
o Certified registered nurse anesthetists;
o Clinical nurse specialists;
o Clinical psychologists;
o Clinical social workers;
o Independently practicing occupational therapists;
o Independently practicing physical therapists;
o Nurse practitioners; and
o Physician assistants.
Eligibility Guidelines
All individuals who are eligible for premium-free Part A are eligible to enroll in Part B. Since Part B is a voluntary program that requires the payment of a monthly premium, those individuals who do not want coverage may refuse enrollment. An individual age 65 years or over who is not eligible for premium-free Part A must be a U.S. resident and either a citizen or an alien lawfully admitted for permanent residence who has resided in the U.S. continuously for the five-year period immediately preceding the month the
Part B enrollment application is filed. Individuals who refused Part B and those whose Part B coverage terminated may enroll or re-enroll in Part B only during prescribed enrollment periods
For Medicare part A eligibility guidelines see the previous post.
Medicare part b covered services
What does Medicare Part B cover?
Medicare Part B helps pay for:
Medicare Part B helps pay for:
- Doctors' services.
- Durable medical equipment (DME) if medical in nature and bought or rented from a Medicare-certified provider.
- Ambulance services when the emergency transportation is from your home to the nearest hospital or skilled nursing facility (SNF) that can provide the necessary services, or from a hospital or SNF to your home, or from one facility to another, and any other type of transportation would endanger your health. Medicare Part B also covers paramedic intercept services in rural areas and regularly scheduled, non-emergency transport when your doctor certifies it.
- Some preventive care services.
- Outpatient physical, speech, and occupational therapy services provided by a Medicare-certified physical, speech, or occupational therapist.
- The first three pints of blood you need each year.
- Chiropractic care when manipulation of the spine is medically necessary to fix a subluxation of the spine. A subluxation is when one or more of the bones of the spine move out of position.
- Outpatient mental health services.
- Home health services if you are homebound and have a skilled nursing need.
- X-rays and lab tests.
- A few prescription drugs, such as immunosuppresant drugs, anti-cancer drugs, anti-emetic drugs, some dialysis drugs and physician-administered drugs that are usually not self-administered.
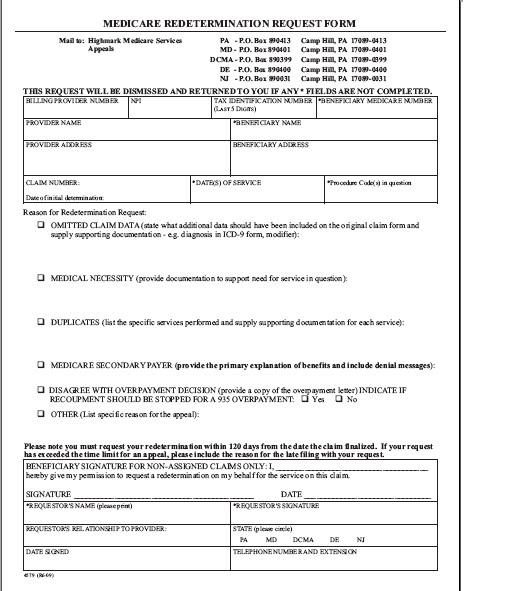
Request for Part B Reconsideration - Example form
Request for Part B Reconsideration by a Qualified Independent Contractor (QIC)


Example Part B Redetermination Request Form
Before you appeal a claim or request a redetermination
Before you file an appeal:
1. Have you checked claims status via SPOT or the IVR?
2. Do you have a SPOT account? If not, get one.
3. Was your claim returned as unprocessable? Here’s how to correct it.
4. Have you reviewed the remittance advice to find out why the claim was not paid, or not paid in full?
5. Is there an opportunity to do a clerical reopening?
Issue
Each month, thousands of medical providers send written inquiries to First Coast Service Options Inc. (First Coast) to check the status of an appealed claim. Unfortunately, many of these appeals and subsequent inquiries are submitted on claims that were ineligible for appeal. Because of this, many providers experience a delay in payment and exhaust valuable time as the process of giving each inquiry its due attention can take up to 60 days.
In fact, most of providers in this scenario would have received payment sooner had they used one of First Coast’s web tools before they mailed their request for a redetermination.
Alternative solutions
1. Check the status of the claim and reason codes first
Claims returned as unprocessable cannot be appealed. Unprocessable claims are returned with the MA130 remittance advice message and a corresponding reason code message to denote why the claim was incomplete or invalid. First Coast offers this information for you to resolve this problem.
Before requesting a redetermination (first level of appealing a Medicare claim), check current claims status via SPOT (Secure Provider Online Tool) or the Part B interactive voice response (IVR) system. In addition, review your remittance advice to find out why payment on a claim may have been reduced or denied.
Many claim redetermination requests can be avoided by reviewing the reason for your claim denial to see if you can resubmit the claim through as a clerical reopening.
2. Transposed dates of service and other clerical errors are easily corrected
Correcting information on claims returned as unprocessable (RUC) and resubmitting the claim is one way to avert lengthy delays in payment. Other claim issues can be resolved without having to request a redetermination or appeal. If a claim was accepted then denied, it is possible a clerical error could have occurred such as a transposed procedure or diagnostic code, inaccurate data entry of a provider number, a modifier, or the date of service. These errors can be corrected through a clerical reopening of the claim.
First Coast offers multiple ways to complete a clerical reopening. If you use SPOT, you may be able to correct such information immediately and avoid a delay in payment.
In some cases, a claim may have been denied as a duplicate claim when it would have otherwise been paid had the correct modifier been submitted with it. Here is how one provider used the SPOT to review a denied claim and correct it.
3. Your claim denial may have gotten caught up with a processing issue
As Medicare policy and procedures change, sometimes electronic processing of claims lags behind these policy changes. First Coast reprocesses claims brought to its attention when errors are made in the electronic processing of claims. First Coast offers a sortable table of current processing issues that may have affected the processing of your claim. The table lets you know if any action is required on your part to have a claim reviewed when a processing issue affects it.
4. Check the status of your appeal
Using the First Coast website, you can confirm that First Coast has received your redetermination request. The appeals confirmation search tool allows you to search by your PTAN to confirm your submission has been received by First Coast. Confirming submission can help prevent the filing of duplicate redetermination requests
Part B Re-determination Request (Form 4579)

Before you file an appeal:
1. Have you checked claims status via SPOT or the IVR?
2. Do you have a SPOT account? If not, get one.
3. Was your claim returned as unprocessable? Here’s how to correct it.
4. Have you reviewed the remittance advice to find out why the claim was not paid, or not paid in full?
5. Is there an opportunity to do a clerical reopening?
Issue
Each month, thousands of medical providers send written inquiries to First Coast Service Options Inc. (First Coast) to check the status of an appealed claim. Unfortunately, many of these appeals and subsequent inquiries are submitted on claims that were ineligible for appeal. Because of this, many providers experience a delay in payment and exhaust valuable time as the process of giving each inquiry its due attention can take up to 60 days.
In fact, most of providers in this scenario would have received payment sooner had they used one of First Coast’s web tools before they mailed their request for a redetermination.
Alternative solutions
1. Check the status of the claim and reason codes first
Claims returned as unprocessable cannot be appealed. Unprocessable claims are returned with the MA130 remittance advice message and a corresponding reason code message to denote why the claim was incomplete or invalid. First Coast offers this information for you to resolve this problem.
Before requesting a redetermination (first level of appealing a Medicare claim), check current claims status via SPOT (Secure Provider Online Tool) or the Part B interactive voice response (IVR) system. In addition, review your remittance advice to find out why payment on a claim may have been reduced or denied.
Many claim redetermination requests can be avoided by reviewing the reason for your claim denial to see if you can resubmit the claim through as a clerical reopening.
2. Transposed dates of service and other clerical errors are easily corrected
Correcting information on claims returned as unprocessable (RUC) and resubmitting the claim is one way to avert lengthy delays in payment. Other claim issues can be resolved without having to request a redetermination or appeal. If a claim was accepted then denied, it is possible a clerical error could have occurred such as a transposed procedure or diagnostic code, inaccurate data entry of a provider number, a modifier, or the date of service. These errors can be corrected through a clerical reopening of the claim.
First Coast offers multiple ways to complete a clerical reopening. If you use SPOT, you may be able to correct such information immediately and avoid a delay in payment.
In some cases, a claim may have been denied as a duplicate claim when it would have otherwise been paid had the correct modifier been submitted with it. Here is how one provider used the SPOT to review a denied claim and correct it.
3. Your claim denial may have gotten caught up with a processing issue
As Medicare policy and procedures change, sometimes electronic processing of claims lags behind these policy changes. First Coast reprocesses claims brought to its attention when errors are made in the electronic processing of claims. First Coast offers a sortable table of current processing issues that may have affected the processing of your claim. The table lets you know if any action is required on your part to have a claim reviewed when a processing issue affects it.
4. Check the status of your appeal
Using the First Coast website, you can confirm that First Coast has received your redetermination request. The appeals confirmation search tool allows you to search by your PTAN to confirm your submission has been received by First Coast. Confirming submission can help prevent the filing of duplicate redetermination requests
Part B Re-determination Request (Form 4579)
Why patient need to get enrolled in Medicare -
Disadvantages of NOT Enrolling in Medicare Part B
Applies only if you are covered for Medicare Part A, but not enrolled in Medicare Part B, and have a medical plan:
- If you decide not to purchase Medicare Part B when you become eligible, your plan will not coordinate coverage for Medicare Part B services. That means you’ll continue to pay for those services and equipment as you did before you become eligible for Medicare. For example, under the Anthem Blue Cross Plan II, a doctor’s office visit will be covered at 80 percent after your deductible. You would be responsible for the remaining 20 percent.
- Without Medicare Part B, you would continue to incur these costs until you hit your out-of-pocket maximum on Anthem Blue Cross Plan II ($2,500 per calendar year, including deductible). If you have Anthem Blue Cross Plan I or Prudent Buyer Plan, you will continue to incur the costs into the future because there is no out-of-pocket maximum.
- You are subject to the one (1) million dollar Lifetime Maximum coverage for the Anthem Blue Cross Plans I, II, and Prudent Buyer Plan, alone or combined. “Combined” means any benefits paid under a prior LACERA-administered Anthem Blue Cross plan will reduce any maximum amounts eligible for the current Anthem Blue Cross plan.
- Without Medicare Part B, you are ineligible to enroll in a LACERA-administered Medicare plan. Thus, you are disqualified from participating in the County’s Medicare Part B Premium Reimbursement Program.
- If you are eligible, but are not enrolled in Medicare Part B and have a HMO plan, you may pay a higher premium.
- Finally, if you decide not to enroll in Medicare Part B when you become eligible at age 65, and later decide to enroll, you will be charged a penalty of 10 percent for each year you were eligible and chose to decline coverage. If you are a late enrollee in Medicare Part B and pick one of the plans eligible for reimbursement, the County will not reimburse the penalty portion of the Part B premium.
Ultimately, the decision is yours. It is worth considering enrolling in Medicare Part B as soon as you are eligible to avoid penalties for late enrollment. Additionally, enrolling in Medicare Parts A and B and a Medicare plan will qualify you for the County’s Medicare Part B Premium Reimbursement Program and coordination of benefits with Medicare, providing the following conditions are met:
- You are paying for your Medicare Part B premium yourself.
- You are not being reimbursed for your Medicare Part B Premium by another agency, for example: other employer, State.
NOTE: Some benefit information mentioned above may be subject to future changes.
Advantages of Enrollment in Medicare Part B
Advantages of Enrollment in Medicare Part B
If you are enrolled in Medicare Parts A and B, and Non-Medicare plan:
- Suppose you have Part B and are enrolled in Anthem Blue Cross Prudent Buyer or Anthem Blue Cross I, II Plan; Medicare and Anthem Blue Cross will coordinate coverage for services. That means when you visit your doctor, once you’ve met your deductible, Medicare Part B will pay 80 percent of eligible services and Anthem Blue Cross will pay a portion of the remaining balance of eligible services, according to each plan design. That leaves you with a small out-of-pocket expense. Over time, Medicare Part B may help reduce your overall health care spending depending how often you use the covered services.
- You are subject to the Lifetime Benefit Maximum of one (1) million dollars coverage for Anthem Blue Cross Plans I, II, and Prudent Buyer Plan, alone or combined. “Combined” means any benefits paid under a prior Anthem Blue Cross plan will reduce any maximum amounts eligible for the current Anthem Blue Cross plan. With Part B coverage paying most of your eligible medical services, it will help you reach your Maximum Lifetime Benefit at a slower pace.
- If you have a Non-Medicare HMO plan, you agree to receive covered services from the plan; and in most situations there is no coordination of coverage between your Medicare and the HMO plan
If you are enrolled in Medicare Parts A and B, and a LACERA-administered Medicare plan:
- Suppose you have both Medicare Part B and Anthem Blue Cross III Plan; Medicare and Anthem Blue Cross will coordinate coverage for services. That means when you visit your doctor, Medicare Part B will pay 80 percent of eligible services and the Anthem Blue Cross III Plan will pick up the remaining 20 percent of eligible services. That leaves little or nothing for you to pay out-of-pocket. Over time, Medicare Part B may help reduce your overall health care spending. In addition, you are not subject to the Lifetime Benefit Maximum of one (1) million dollars that applies to the other Anthem Blue Cross plans.
- If you have a LACERA-administered Medicare Advantage Prescription Drug Plan (MA-PD) such as Kaiser Senior Advantage, you assign Medicare Parts A, B, and D to your medical plan, and must receive all covered services directly from the plan.
- Currently, the County reimburses the 2008 Medicare Part B standard rate of $96.40 for all Medicare Plan enrollees, subject to annual review and approval by the Board of Supervisors.
Medicare part b benefits - who is eligible.
How You Get Part B
- If you get benefits from Social Security or the Railroad Retirement Board (RRB), in most cases you'll automatically get Part B starting the first day of the month you turn 65. If your birthday is on the first day of the month, your Part B will start the first day of the prior month.
- If you're under 65 and disabled, you'll automatically get Part B after you get disability benefits from Social Security or certain disability benefits from the RRB for 24 months. You’ll get your Medicare card in the mail about 3 months before your 65th birthday or your 25th month of disability.
- If you don't want Part B, follow the instructions that come with the card, and send the card back. If you keep the card, you keep Part B and will pay Part B premiums.
- If you have ALS (Amyotrophic Lateral Sclerosis, also called Lou Gehrig’s disease), you automatically get Part B the month your disability benefits begin.
Medicare part B covered services
Medicare Part B Benefits (Medical Insurance)
What Is Part B (Medical Insurance)?
Part B helps cover medically-necessary services like doctors' services, outpatient care, home health services, and other medical services. Part B also covers some preventive services. Check your Medicare card to find out if you have Part B.
How Much Does Part B Cost?
You pay the Part B premium each month. Most people will pay the standard premium amount (link to current amount?. However, if your modified adjusted gross income as reported on your IRS tax return from 2 years ago is above a certain amount, you may pay more.
Your modified adjusted gross income is your taxable income plus your tax exempt interest income. Social Security will notify you if you have to pay more than the standard premium. If you have to pay a higher amount for your Part B premium and you disagree (even if you get Railroad Retirement Board benefits), call Social Security at 1-800-772-1213. TTY users should call 1-800-325-0778.
If you don't sign up for Part B when you are first eligible, you may have to pay a late enrollment penalty.
What Is Part B (Medical Insurance)?
Part B helps cover medically-necessary services like doctors' services, outpatient care, home health services, and other medical services. Part B also covers some preventive services. Check your Medicare card to find out if you have Part B.
How Much Does Part B Cost?
You pay the Part B premium each month. Most people will pay the standard premium amount (link to current amount?. However, if your modified adjusted gross income as reported on your IRS tax return from 2 years ago is above a certain amount, you may pay more.
Your modified adjusted gross income is your taxable income plus your tax exempt interest income. Social Security will notify you if you have to pay more than the standard premium. If you have to pay a higher amount for your Part B premium and you disagree (even if you get Railroad Retirement Board benefits), call Social Security at 1-800-772-1213. TTY users should call 1-800-325-0778.
If you don't sign up for Part B when you are first eligible, you may have to pay a late enrollment penalty.
Subscribe to:
Posts (Atom)
Top Medicare billing tips
-
 CPT CODES and Description 81000 Urinalysis, by dip stick or tablet reagent for bilirubin, glucose, hemoglobin, ketones, leukocytes, nitr...
CPT CODES and Description 81000 Urinalysis, by dip stick or tablet reagent for bilirubin, glucose, hemoglobin, ketones, leukocytes, nitr... -
CPT Codes for Laceration Repair Laceration Simple/Superficial-Scalp, Neck, Axillae, External Genitalia, Trunk, Extremities : 2.5 cm o...
-
procedure code and description 93922 LIMITED BILATERAL NONINVASIVE PHYSIOLOGIC STUDIES OF UPPER OR LOWER EXTREMITY ARTERIES, (EG, FOR LOW...
-
Frequency Limitations: Testing may be covered up to two times a year in clinically stable patients; more frequent testing may be reasonabl...
-
CPT CODE and Description • 99401 – preventive medicine counseling and/or risk factor intervention/s provided to an individual (separate pro...
-
 Procedure Codes and Definitions 36415 Collection of venous blood by venipuncture - Fee schedule amount $3.10 - Private insurance pay upt...
Procedure Codes and Definitions 36415 Collection of venous blood by venipuncture - Fee schedule amount $3.10 - Private insurance pay upt... -
Patient Discharge Status Code - Definition A patient discharge status code is a two-digit code that identifies where the patient is at th...
-
 CPT CODE and description 99243 - Office consultation for a new or established patient, which requires these 3 key components: A detailed h...
CPT CODE and description 99243 - Office consultation for a new or established patient, which requires these 3 key components: A detailed h... -
Procedure Code Changes and Description • Deleted Codes * 49080 - Peritoneocentesis, abdominal paracentesis, or peritoneal lavage (diagnostic...
-
Coding Code Description CPT E0218 Water circulating cold pad with pump E0236 Pump for water circulating pad E0650 Pneumatic Compressor,...